
You’ve had the standard work-up. Maybe coeliac disease was ruled out. Maybe your IgE allergy testing came back negative. Yet the bloating still builds through the afternoon, the headaches arrive without a clear pattern, and your skin or joints seem to flare for reasons you can’t pin down.
That’s the point where many people start searching for an igg allergy test. Not because they want a trendy wellness shortcut, but because they want a structured way to investigate delayed food reactions when the obvious causes haven’t explained the whole picture.
Used badly, IgG testing creates confusion and over-restriction. Used properly, inside a practitioner-led process with clinical history, serum collection, and a disciplined elimination and reintroduction plan, it can become a useful piece of the puzzle.
Understanding Your Unexplained Symptoms
A common clinical pattern looks like this. Someone feels “off” most days, but not acutely unwell. They eat reasonably well, they’ve tried cutting out one or two foods on their own, and they still can’t work out why they feel swollen, foggy, tired, or inflamed.

The difficulty is timing. Not all food reactions are immediate. If a food gives you symptoms hours later, or even the next day, it’s much harder to connect the reaction to the meal that triggered it. Patients often tell me they’ve kept a mental note of problem foods, but the pattern never feels clean enough to trust.
In Australia, food intolerances and allergies affect approximately 20% of the population, while true IgE-mediated allergies comprise less than 10% of cases, which points to a substantial burden of non-IgE mediated reactions that may be harder to identify through standard allergy pathways, according to ARUP reference interval material.
Why symptoms can feel random
Delayed reactions don’t behave like classic allergies. They don’t usually announce themselves within minutes. Instead, people report patterns such as:
- Digestive drift. You wake up fine, then become bloated after lunch and uncomfortable by dinner.
- Low-grade inflammation. Headaches, fatigue, sinus pressure, skin flare-ups, or achy joints come and go.
- Food confusion. You remove one suspected trigger, feel slightly better, then plateau because other triggers remain.
Sometimes the biggest clue isn’t one dramatic reaction. It’s the repetition of small symptoms that never fully switch off.
When symptoms overlap with IBS-style digestive complaints, a structured dietary approach can also help narrow the field. For some people, resources on a FODMAPs diet for SIBO are useful alongside clinical assessment, especially when bloating and fermentation symptoms dominate.
When testing enters the conversation
An igg allergy test isn’t meant to replace clinical judgement. It’s an investigative tool for people whose symptoms suggest food may be involved, but whose response doesn’t fit the classic allergy picture.
That distinction matters. If your symptoms are delayed, chronic, and difficult to map, testing can help move the conversation from guesswork to a more organised elimination strategy.
The Science of Food Reactions IgG vs IgE
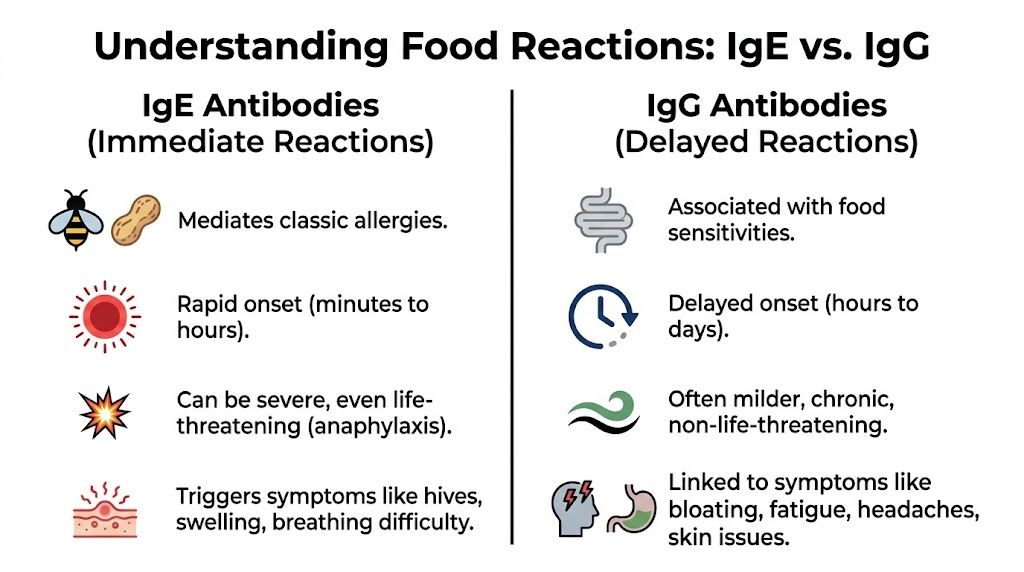
When people say “allergy test”, they’re often talking about IgE. That’s the antibody involved in classic immediate allergic reactions. Think hives, swelling, wheeze, throat symptoms, or more severe reactions that can escalate quickly.
IgG is different. In the food sensitivity discussion, increased food-specific IgG is used as a marker that may point toward a delayed immune response pattern rather than an acute allergy. The practical difference is timing, symptom style, and how results should be used.
A simple way to think about it
IgE is the sudden fire alarm. It tends to trigger quickly and loudly.
IgG is more like a slow-burn signal. If it matters clinically, it often shows up as ongoing irritation rather than an obvious emergency. That’s why people can eat the same foods for years and still struggle to identify what’s aggravating them.
IgE allergy vs IgG intolerance at a glance
| Attribute | IgE-Mediated Allergy (Type I) | IgG-Mediated Intolerance (Type III) |
|---|---|---|
| Typical timing | Minutes to hours | Hours to days |
| Reaction pattern | Immediate and often obvious | Delayed and harder to track |
| Common symptom style | Hives, swelling, breathing symptoms | Bloating, headaches, fatigue, skin issues, joint discomfort |
| Clinical concern | Can be severe or life-threatening | Usually chronic and non-emergency in presentation |
| How results are used | Allergy diagnosis and risk management | Guided elimination and reintroduction planning |
Why standard allergy testing can miss the issue
If a patient’s symptoms come on the next morning, or after repeated exposure through the week, an IgE test may not explain much. That doesn’t mean symptoms are imaginary. It means the immune pathway may be different, or food may be contributing in a less direct but still meaningful way.
Another detail practitioners look at is the underlying measurement. Clinical-grade serum assays quantify food-specific IgG antibodies. Reference benchmarks from ARUP indicate that values below 2.00 mcg/mL are considered absent or undetectable, while results above that threshold may indicate a potential reaction pattern when interpreted in context through ARUP’s ImmunoCAP test information.
Practical rule: An IgG result on its own doesn’t prove a food is the problem. The result becomes useful when it matches the patient’s symptoms, history, and response to a structured dietary trial.
What the science does and doesn’t support
Many articles provide an overly simplistic explanation. IgG isn’t a tool for diagnosing anaphylactic food allergy. It should never be used that way.
Its clinical use sits elsewhere. In practice, it can help identify which foods deserve a carefully supervised trial removal when the symptom picture suggests delayed intolerance rather than immediate allergy.
Clinical Validity and Practitioner Perspectives
The debate around IgG testing is real, and patients deserve a straight answer about it.

The Royal Australian College of General Practitioners (RACGP) and Australasian Society of Clinical Immunology and Allergy (ASCIA) do not endorse IgG panels for food intolerance diagnosis, as noted in the AAAAI overview on IgG food testing. That position is important. It reflects the fact that IgG testing shouldn’t be presented as a stand-alone diagnosis of food allergy.
Where scepticism is justified
There are several ways IgG testing gets misused:
- As a diagnostic shortcut. A report is treated as the final answer rather than the beginning of an investigation.
- Without symptom correlation. Foods are removed only because they appear on a list.
- Without nutritional oversight. Patients end up on highly restrictive diets that are hard to sustain and may do more harm than good.
Those criticisms are fair. I share them.
Where the test can still be useful
The more useful clinical question isn’t “Is IgG testing perfect?” It isn’t. The better question is whether it can help guide a targeted elimination protocol in patients with persistent symptoms and no clear explanation from standard assessment.
That’s where practitioner skill matters. If I use this kind of testing, I’m not asking the report to diagnose the patient. I’m asking it to help prioritise foods for a structured trial so we can observe what changes and what doesn’t.
For a balanced discussion of that issue, the article on whether IgG food intolerance testing is reliable is worth reviewing alongside clinical judgement and symptom history.
A helpful overview is below.
The standard I use in practice
A clinically responsible approach usually includes:
- Ruling out red flags first. Immediate allergy, coeliac disease, inflammatory bowel disease, and other significant pathology need attention before food sensitivity testing enters the picture.
- Using the results as a map, not a verdict. The report helps organise the dietary trial.
- Testing the hypothesis. If removing the most reactive foods changes nothing, the answer likely lies elsewhere.
Good practitioners don’t ask patients to fear food. They use testing to reduce unnecessary guesswork.
The ImuPro Process A Clinical-Grade Approach
The reliability of an igg allergy test depends heavily on how the sample is collected and processed. That point gets missed in many online discussions.
For clinical use, I favour venous blood draw with serum analysis through a pathology collection process. That gives better control over specimen handling than informal home collection methods. It also means the sample enters an established clinical chain from collection to transport.
Why serum collection matters
With serum-based testing, the practical concern is stability. According to ARUP’s test methodology information, food-specific IgG testing can be performed on serum, and serum stability can extend up to 2 weeks when refrigerated if handled appropriately. That matters when samples need to move safely from a local collection centre to a specialised laboratory.
This is one of the clearest distinctions between a clinical-grade process and a convenience-first model. Better pre-analytical handling usually means fewer variables before the lab even starts measuring antibodies.
What happens after the blood draw
The workflow is straightforward:
- Pathology collection. A venous blood sample is taken at a collection centre.
- Serum preparation and transport. The sample is handled for laboratory analysis under controlled conditions.
- ELISA analysis. Food-specific IgG antibodies are quantified using validated laboratory methods.
- Report generation. The clinician receives a food reactivity profile to interpret alongside symptoms and diet history.
One option used in Australian practice is ImuPro, which analyses food-specific IgG antibodies in ISO-certified ELISA laboratories in Germany and offers tiered panels ranging from smaller screens to broader food coverage. Depending on the panel, testing can assess 22 to 270 antigens, and IgG levels above 2.00 mcg/mL are treated as a potential reaction marker rather than a diagnosis in itself, based on the same ARUP benchmark framework.
Choosing panel breadth sensibly
Bigger isn’t always better. The right panel depends on diet variety, symptom complexity, and whether there are special dietary patterns involved.
A practical way to think about panel selection is:
| Situation | Sensible approach |
|---|---|
| Narrow diet, clear suspects | Start with a smaller panel to identify likely priorities |
| Broad diet, long symptom history | A wider panel may save time by reducing repeated guesswork |
| Vegetarian or restricted eating pattern | Choose a panel that reflects actual food exposure |
What works better than broad food avoidance
The best testing process still fails if the follow-up plan is poor. I’ve seen patients remove too many foods too quickly, then become anxious around eating. That usually tells me the process wasn’t managed well.
A useful test should support a more precise intervention. It should narrow the trial, not expand the confusion.
Interpreting Your Results For Actionable Change
Patients typically don’t struggle with the blood test. They struggle with the report.
A page of reactive foods can make anyone feel they’ve suddenly lost their normal diet. That isn’t how I’d want you to read it. The report is not a permanent ban list. It’s a working document for a phased food trial.

Phase one is elimination
The first phase is temporary removal of the foods showing the strongest reactivity, but only within a plan that still leaves you enough variety and nutrition.
This phase works best when patients keep things simple:
- Record symptoms clearly. Note digestion, energy, skin, sleep, headaches, and joint changes.
- Don’t keep changing the plan. If you remove five foods and add supplements, probiotics, and fasting all at once, you won’t know what helped.
- Keep meals realistic. If dairy is out, practical guides to protein lactose-free options can help maintain food variety while you test the response.
Phase two is provocation
Once symptoms have settled, foods are reintroduced systematically. Many people learn during this reintroduction that not every reactive food creates the same effect.
One food may clearly reproduce bloating or headaches. Another may be tolerated once the system has calmed down. That’s why a result sheet should never be treated as a final life sentence.
The reintroduction phase is where the useful answers usually appear. Without it, you only know what you removed, not what truly matters.
Phase three is rotation
Rotation isn’t about perfection. It’s about avoiding constant repetition of foods that may have contributed to immune activation in the first place.
A long-term plan often looks like this:
- Confirmed triggers stay out for longer while the gut and symptom picture stabilise.
- Borderline foods return in moderation if they don’t recreate symptoms.
- Diet variety improves over time rather than shrinking further.
How to read the report sensibly
A practical interpretation usually follows these rules:
| Report feature | How to think about it |
|---|---|
| Higher reactivity | Prioritise for initial elimination if symptoms fit |
| Mild reactivity | Consider context, frequency of eating, and symptom relevance |
| No clear symptom match | Don’t overreact. Monitor rather than assume |
| Large number of reactive foods | Step back and build a realistic plan with practitioner guidance |
The most productive mindset is curiosity, not fear. We’re asking, “What changes when this food is removed and then reintroduced?” That’s a much better question than “Which foods are bad?”
Beyond Food IgG The DAO and Histamine Connection
Some patients do a careful food elimination and still feel that the picture doesn’t fully add up. They react to leftovers, wine, aged foods, fermented foods, or meals that seem inconsistent from one day to the next. That’s when I start thinking more carefully about histamine.
Histamine symptoms can overlap with delayed food reactions. People may report bloating, headaches, flushing, skin symptoms, fatigue, or a sense that certain foods are problematic but not in a predictable allergy pattern. In those cases, food IgG alone may not explain everything.
Why the overlap matters
DAO, or diamine oxidase, is the enzyme involved in breaking down histamine from foods. If DAO function is low, high-histamine foods can become an extra burden. The result is a mixed picture that’s easy to misread as “random food intolerance”.
Australian interest in this overlap has grown because one Melbourne pilot found that 68% of histamine-intolerant patients had co-occurring high IgG to fermented foods, according to ADLM’s clinical utility discussion referenced in the Australian context.
When combined assessment is useful
Combined assessment tends to make sense when:
- Fermented foods are a repeated issue. Think cheese, yeast-containing foods, or other aged items.
- Symptoms are broad and inconsistent. The patient can’t identify one clear trigger pattern.
- IgE testing was unrevealing. The immediate allergy pathway doesn’t explain the experience.
For patients exploring that angle, guidance on how to test for histamine intolerance can help frame whether DAO assessment belongs in the work-up.
If your symptoms worsen with fermented or aged foods, the question may not be only “Which foods am I reacting to?” It may also be “What am I struggling to break down?”
Frequently Asked Questions About IgG Testing
Is an igg allergy test the same as an allergy diagnosis
No. That’s the most important clarification. IgG testing is not used to diagnose classic food allergy. It’s used, at most, as part of a broader assessment for delayed food intolerance patterns and to guide a supervised elimination and reintroduction process.
Will I need to avoid these foods forever
Usually not. In most cases, the goal is temporary removal, symptom observation, and then careful reintroduction. Some foods may prove to be genuine ongoing triggers, while others can often return once the system settles.
Why isn’t it covered by Medicare
Because it sits outside standard endorsed pathways for diagnosing food allergy. In Australia, these tests are generally accessed privately as complementary investigations rather than routine Medicare-funded diagnostics.
What does rotation actually mean in daily life
It means avoiding the same reactive or borderline foods every day. Instead of repeating one staple constantly, you vary your food choices across the week. That can reduce overexposure and gives you more useful feedback about what you tolerate.
How quickly will I notice a difference
That varies. Some people notice changes fairly early. Others need a more disciplined trial before the pattern becomes obvious. What matters most is running the process cleanly enough that the result means something.
Who is a poor candidate for this kind of testing
People with suspected immediate allergy symptoms need a conventional allergy work-up first. It’s also not a good starting point for someone who is already highly restrictive, underweight, medically unstable, or prone to obsessive food avoidance unless there is close clinical support.
What makes one testing pathway more reliable than another
The quality of the process. In practice, that means proper clinical screening, venous blood collection through pathology, serum handling, validated laboratory methods, and skilled interpretation. The test alone isn’t the intervention. The value comes from how the results are used.
If you’ve exhausted the obvious options and still suspect food is contributing to persistent symptoms, ImuPro Australia offers a clinical-grade, serum-based pathway that can be used as part of a structured practitioner-led investigation rather than a stand-alone shortcut.