
Fatigue that doesn’t lift. Brain fog by mid-morning. Hair shedding, low mood, poor exercise recovery, or the sense that your body isn’t quite keeping up. These symptoms are common, but they’re also frustrating because they can come from many different causes. A blood test for vitamins and minerals deficiencies australia can help move the discussion away from guesswork and towards something objective.
That matters because nutrient testing works best when it’s treated as a clinical tool, not a wellness trend. The most reliable approach is a venous blood draw collected at a pathology centre, where sample handling, transport, and laboratory processing follow established clinical standards. That’s very different from consumer tests that prioritise convenience over specimen quality.
Your Guide to Vitamin and Mineral Blood Testing in Australia
A good nutrient blood test doesn’t diagnose every cause of fatigue or poor wellbeing. It does something more useful. It tells you whether key nutrients look adequate, borderline, or low enough to warrant a proper management plan.
In practice, the value of testing depends on asking the right question. If someone feels run down after a period of stress, a small, focused panel may be appropriate. If symptoms are ongoing, broad, or difficult to explain, a practitioner may look more widely at vitamins, minerals, and related markers to understand whether a deficiency pattern is part of the picture.
Why clinical-grade collection matters
For this topic, the method matters as much as the marker. A venous sample collected through a pathology service gives the laboratory enough high-quality specimen to run validated assays and repeat analysis if needed. It also reduces many of the pre-analytical problems that can distort results.
Practical rule: If you want results you can confidently discuss with your GP, dietitian, or naturopath, start with a pathology-collected venous blood draw.
Clinical-grade testing is also easier to integrate into real care. Your practitioner can compare results with your symptoms, medications, diet, medical history, and any previous pathology. That context is where interpretation becomes useful.
What sensible testing looks like
The best approach is usually straightforward:
- Start with symptoms and history: Fatigue, poor concentration, recurrent infections, low mood, muscle aches, or restricted eating patterns all change what should be tested.
- Use a pathology collection centre: That protects sample quality and gives the lab a proper venous specimen.
- Interpret results clinically: Numbers alone don’t tell the whole story. Recent supplements, illness, and timing of the test can all influence what appears on the report.
A blood test is a starting point. Its value is realised when the result leads to a targeted next step rather than more confusion.
Identifying Key Nutrients Measured in Blood Tests
Not all “vitamin tests” are the same. Some are narrow and practical. Others are broad panels designed to examine several nutrient systems at once. The right test depends on symptoms, diet, medications, and how much clinical detail is needed.
Common nutrients practitioners look at
A standard work-up often focuses on nutrients that are both clinically relevant and commonly discussed in general practice:
- Vitamin D: Frequently assessed in people with fatigue, low sun exposure, or bone and muscle concerns. For a plain-language overview, this Information on vitamin D testing gives a useful summary of what the marker is trying to assess.
- B-group vitamins: Especially B12 and folate when tiredness, poor concentration, dietary restriction, or neurological symptoms are part of the story.
- Iron-related markers: Often checked when fatigue, shortness of breath on exertion, heavy menstrual bleeding, or hair loss are present.
- Minerals such as magnesium, zinc, copper, selenium, and calcium: These may be considered when symptoms are broader or when a practitioner suspects dietary insufficiency, malabsorption, or chronic metabolic stress.
Some results reflect immediate circulation in the blood. Others are chosen because they can give a better sense of tissue status or longer-term balance.
Standard panels and advanced panels
There’s a big difference between a focused GP request and an extensive private panel. According to Australian advanced nutrient panel descriptions, the most extensive vitamin and mineral blood test panels can assess over 240 biomarkers, while a more targeted Core Nutrients Test measures 17 biomarkers and includes markers such as activated B12 and red blood cell mineral status.
That distinction matters. A focused panel is often enough when the clinical question is narrow. A broader panel may be more useful when symptoms are persistent, when previous basic testing hasn’t clarified much, or when a practitioner wants a wider metabolic view.
Broad testing isn’t automatically better. Better testing is testing that matches the clinical question.
A full panel may also include organic acids, which can show downstream effects of nutrient insufficiency on metabolism. That can be helpful when a practitioner is looking beyond a single low nutrient and trying to understand functional consequences.
Where people get confused
Many patients assume every nutrient test measures the same thing in the same way. It doesn’t. One laboratory may report serum nutrients only. Another may include intracellular or red blood cell markers as well.
That’s one reason comparisons with non-blood methods can be misleading. If you’ve come across discussions about alternative approaches, this overview of hair mineral analysis compared with IgG blood serum testing is useful because it highlights why specimen type and laboratory method affect how much confidence you can place in a result.
Prevalent Australian Nutrient Deficiencies and Symptoms
Australia has a strong public health story around nutrient testing, but one issue stands out clearly. Vitamin D deficiency affects approximately 23% of Australian adults, according to the Australian Bureau of Statistics biomedical results. That’s roughly one in four adults.

The same ABS data shows how uneven deficiency can be. Rates rise to 36% in winter and fall to 14% in summer. Winter rates are especially high in southern jurisdictions, including Victoria at 49%, the Australian Capital Territory at 49%, and Tasmania at 43%, while Queensland sits at 15% and the Northern Territory at 17% in winter.
Why symptoms can be vague
Vitamin and mineral deficiencies rarely announce themselves neatly. People usually present with overlapping complaints such as:
- Persistent tiredness: Often described as feeling flat despite sleep.
- Poor concentration or brain fog: Trouble focusing, slower recall, or reduced mental stamina.
- Muscle aches or weakness: Sometimes mild, sometimes enough to affect training or day-to-day activity.
- Frequent minor illnesses: Not proof of a deficiency, but worth discussing if it’s part of a broader pattern.
- Hair thinning or brittle nails: Commonly blamed on stress alone, though nutrition can be part of the picture.
None of these symptoms confirms a deficiency. They justify a more careful review when they persist.
The Australian context matters
Australia’s vitamin D story often surprises patients. People assume a sunny country protects everyone. It doesn’t. Time indoors, sunscreen use, clothing, skin pigmentation, age, and geography all influence vitamin D status.
The ABS report also noted lower deficiency among people taking supplements. Only 5% of adults were taking vitamin D supplements in 2011-12, and deficiency was 7% among supplement users compared with 23% among non-users in that survey period. That doesn’t mean everyone should self-prescribe vitamin D. It does show why testing and individual advice matter.
Symptoms can point towards a nutrient issue, but they can also reflect sleep problems, thyroid disease, infection, stress, medication effects, gut disorders, or low energy intake. Testing helps separate suspicion from evidence.
Iron is also a frequent clinical concern in Australia, particularly when fatigue, hair shedding, low exercise tolerance, or heavy periods are part of the history. But symptoms alone aren’t enough. Two people can describe the same tiredness and have completely different underlying causes. That’s why pathology remains the sensible next step before starting supplements.
Navigating the Pathology Testing Process in Australia
Typically, the testing pathway is simpler than expected. You discuss symptoms with a practitioner, receive a request or choose an appropriate private test, then attend a pathology collection centre for a venous blood draw.
Starting with the request
The GP still sits at the centre of nutrient testing in Australia. In a study of testing trends, vitamin D testing growth in Australia increased 94-fold between 2000 and 2010, and 80% of those tests were ordered by general practitioners. That tells you something important. Nutrient assessment has become routine enough that most GPs are familiar with the process, even if they differ in how broadly they investigate.
If appointment access is the obstacle, systems that improve bookings, triage, and communication can help people move through care more smoothly. Health services exploring Simbie AI patient access solutions are addressing that administrative bottleneck rather than the test itself, but the practical effect is still relevant to patients trying to get assessed promptly.
What happens at the collection centre
At the pathology site, a trained collector confirms your details, checks the request, and takes blood from a vein in your arm. The process is brief. Most patients tolerate it well, especially when they arrive hydrated and seated calmly for a few minutes beforehand.
What usually helps:
- Bring the request details: Paper or digital, depending on the provider.
- Check preparation instructions: Some nutrient markers may have specific timing or fasting instructions set by the requesting practitioner or laboratory.
- Mention supplements and medicines: They can influence interpretation, even when the collection itself is straightforward.
Later, the sample is labelled, processed, and sent through a formal laboratory workflow. That chain of custody is one reason pathology-based venous sampling remains the preferred standard.
A related point often missed is that a proper pathology pathway also protects against over-reading self-collected results. People sometimes compare very different tests as though they were interchangeable. They aren’t. This discussion of a blood type test kit and laboratory testing context is a useful reminder that collection method and lab handling affect what confidence a clinician can place in any result.
Reducing anxiety about the blood draw
Most concerns are practical rather than medical. People worry about needles, fainting, or whether they’ve prepared correctly.
A few simple steps usually make the appointment easier:
- Drink water beforehand: Better hydration often makes veins easier to access.
- Eat if you’ve been told you can: Don’t fast unless the test instructions require it.
- Tell the collector if you’ve fainted before: They can usually position you more comfortably.
- Stay seated briefly afterwards: Especially if you’re anxious or rushing to work.
The process is routine, controlled, and designed for accuracy. That’s exactly what you want when symptoms are already creating uncertainty.
GP Referral vs Direct Access Testing Models
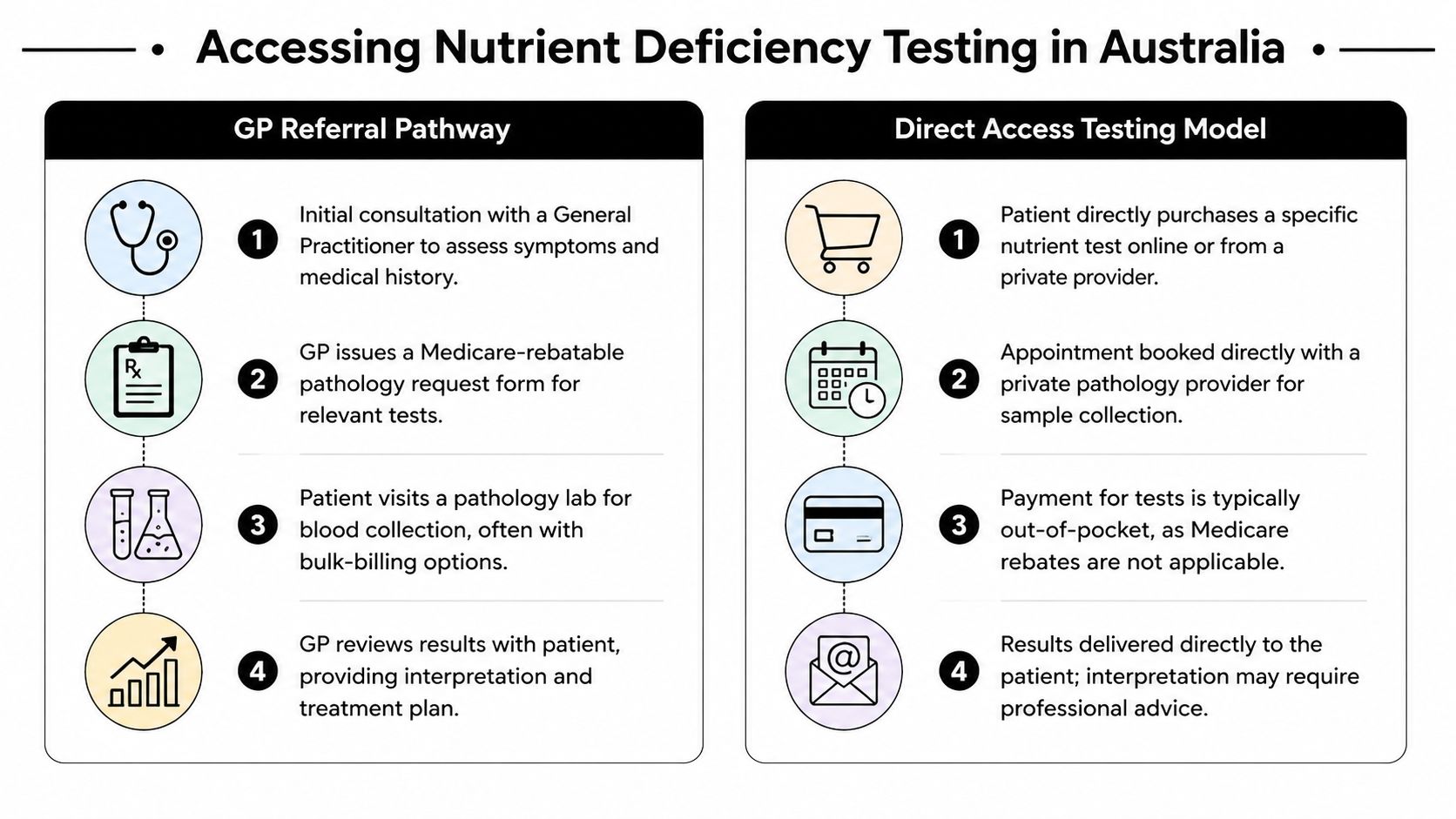
People generally reach nutrient testing through one of two paths. They either see a GP who orders pathology, or they access a private test directly and attend a pathology service for collection. Both models can work well. The better choice depends on what you need from the result.
Side-by-side differences
| Pathway | Best suited to | Main strength | Main limitation |
|---|---|---|---|
| GP referral | People with complex symptoms, medical conditions, medication use, or possible non-nutrient causes | Clinical oversight and integration with broader health care | Test scope may be narrower and shaped by standard practice |
| Direct access private testing | People who want broader nutrient screening or a specific private panel | Greater autonomy and access to specialised options | Results still need professional interpretation and are usually self-funded |
When GP referral is the better first step
If symptoms could reflect something other than deficiency, the GP route is usually safer. That includes unexplained weight loss, persistent gastrointestinal symptoms, significant changes in mood, neurological symptoms, bleeding issues, or marked fatigue that could have many causes.
The GP’s advantage isn’t only the test order. It’s the surrounding clinical judgement. They can decide whether nutrient testing is enough, whether another diagnosis needs to be ruled out, and whether treatment should start immediately or wait for a fuller picture.
This path also helps when your result needs to sit beside prior history, imaging, medications, or specialist letters. In real practice, that context often changes what the numbers mean.
Where direct access can be useful
Private testing suits people who are proactive, informed, and clear about what they’re seeking. It can also be valuable when someone wants a broader nutritional assessment than a standard general practice work-up is likely to provide.
That’s particularly relevant when symptoms are chronic but non-specific, or when someone has already had routine pathology that didn’t fully answer the question. Some private panels include markers that standard pathology requests may not routinely cover, including more detailed nutrient status markers.
A direct-access result is only as useful as the plan that follows it. Good testing gives you data. Good care decides what to do with it.
The practical trade-off
The GP pathway tends to offer stronger medical continuity. The direct-access pathway tends to offer more control over scope and timing. Neither replaces clinical interpretation.
A sensible way to think about it is this:
- Choose GP-led testing if diagnosis is still wide open and you need medical oversight.
- Choose direct access if you already know you want a broader private panel and you’re prepared to review the result with a qualified practitioner.
- Avoid treating any isolated low or borderline value as a complete explanation for complicated symptoms.
Some private providers have moved towards a hybrid approach. The patient initiates access, but the collection still occurs through a clinical pathology network using a venous sample. That’s a stronger model than casual home testing because it preserves specimen quality and laboratory standards.
What works and what doesn’t
What works is a test that answers a real clinical question and feeds into care. What doesn’t work is collecting numbers without context, then self-treating aggressively based on a single marker.
The practical goal isn’t to choose the “better” system in the abstract. It’s to choose the system that gives you accurate collection, appropriate scope, and a path to informed interpretation.
Understanding Your Vitamin and Mineral Test Results
A pathology report can look deceptively simple. There’s a marker name, a number, and a reference range. Patients often assume the key question is whether a result is flagged high or low. In practice, interpretation is more nuanced than that.
Reference range versus clinical meaning
A reference range is the interval the laboratory uses to describe where many results from a broader population tend to fall. It’s useful, but it isn’t the whole clinical story.
A result inside range doesn’t automatically explain symptoms away. A result outside range doesn’t automatically tell you why you feel unwell. Practitioners interpret the number alongside the history, medications, current supplements, diet, and the reason the test was ordered in the first place.
Clinical insight: The same result can mean different things in different people. A supplement user, a person recovering from illness, and a patient with gut symptoms may need very different interpretations of the same laboratory value.
Serum markers and red blood cell markers
For many patients, serum or plasma markers provide significant clarity, generally reflecting what is circulating in the blood at that point in time. They can be influenced by recent intake, recent supplementation, and short-term physiological changes.
Red blood cell or intracellular markers aim to show a longer-term picture. Red blood cells have a lifespan that makes them useful for assessing nutrient status over a more extended period rather than just what is moving through the bloodstream that day.
A simple way to consider it:
| Marker type | What it often reflects | Why it matters |
|---|---|---|
| Serum or plasma | More immediate or recent circulating status | Useful for acute assessment and many standard pathology decisions |
| Red blood cell or intracellular | Longer-term tissue-related status | Useful when symptoms are chronic or when short-term intake may mask a deeper issue |
One common gap in public education is that patients are rarely told when one type is more informative than the other. According to guidance gaps around red cell mineral testing, there is limited consumer-facing explanation of when serum testing is enough, when red blood cell markers add value, and how clinicians should integrate both into decision-making.
That matters in everyday practice. A patient may have a serum marker that looks acceptable after recent dietary effort or supplementation, while a longer-term marker still suggests depletion over time. That doesn’t make one test right and the other wrong. It means they are answering different questions.
Why reports shouldn’t be read in isolation
Several factors can complicate interpretation:
- Recent supplements: These may shift serum values more quickly than deeper tissue status.
- Current illness or inflammation: Acute physiology can alter how some results appear.
- Exercise and timing: A hard training session or poor preparation can affect some markers.
- Laboratory method: Different panels don’t always assess the same biological compartment.
For that reason, “normal” and “optimal for this person” aren’t always identical concepts. Clinicians use the report as one piece of evidence, not a verdict.
If your symptoms are ongoing, ask a better question than “Is this normal?” Ask what the marker measures, whether it reflects short-term or longer-term status, and whether the result fits the rest of your clinical picture.
Actionable Next Steps and Professional Guidance
The useful part of testing starts after the report arrives. A result should lead to a discussion about food intake, sun exposure, medications, digestive health, supplementation, and whether further investigation is needed. For some people, the right next step is dietary change. For others, it’s targeted supplementation and repeat testing. For others again, it’s recognising that symptoms need a broader medical work-up.
If you need a practitioner to help join those dots, this directory-style guide to functional medicine doctors in Australia can be a practical starting point alongside your GP and dietitian.
If you want clinically handled testing that prioritises pathology collection and laboratory rigour, ImuPro Australia offers blood serum-based wellness diagnostics designed to fit into a professional care pathway. The value isn’t in collecting more numbers for their own sake. It’s in getting reliable data you can use in an informed discussion with your healthcare practitioner.