
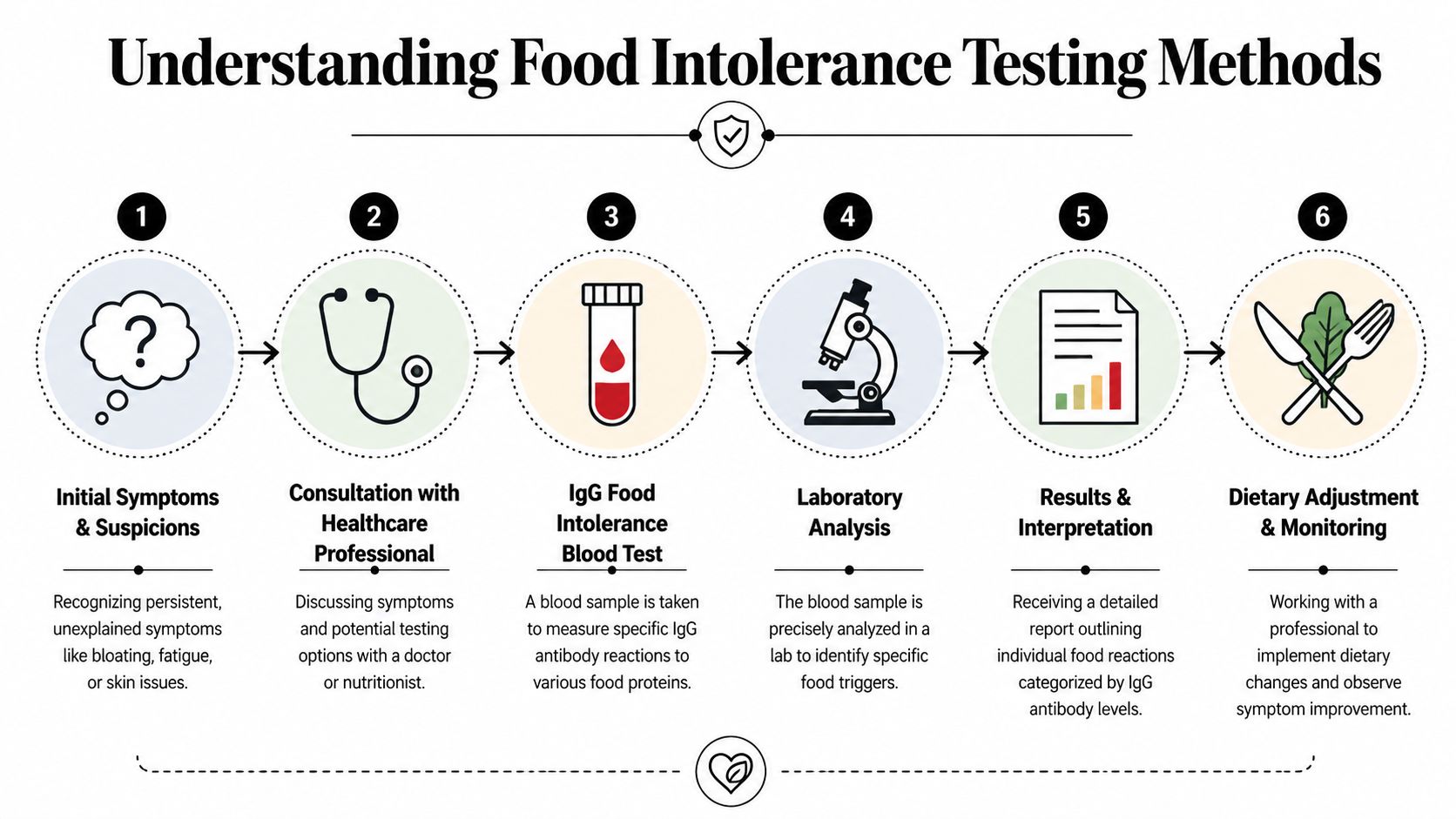
If you're dealing with bloating after meals, headaches that don't seem tied to stress, skin flare-ups, fatigue, or a gut that feels unpredictable, it's reasonable to ask whether food is involved. The difficulty is that chronic food-related symptoms rarely announce themselves clearly. They can appear hours later, vary from day to day, and overlap with other digestive or inflammatory issues.
That’s why learning how to test for food intolerance matters. Good testing isn’t about finding a single magic answer. It’s about using the right clinical tools, in the right order, so you can separate genuine patterns from guesswork and avoid cutting out foods unnecessarily.
Understanding Chronic Symptoms and Food Intolerance
A common clinical scenario looks like this. Someone has months of bloating, headaches, skin flare-ups, or fatigue, has already tried cutting out obvious trigger foods, and still cannot see a reliable pattern. The reason is often timing. Delayed food reactions do not behave like immediate allergies, so the link between a meal and a symptom is easy to miss.

A food allergy usually involves a rapid immune response and can be urgent. A food intolerance is different. In some cases, the clinical picture may include IgG antibodies, with symptoms appearing hours or even days later. That delay is why many people feel sure food is involved but struggle to identify which food, how much, and how often it matters.
Why delayed symptoms are harder to identify
Delayed symptoms create a tracing problem. A reaction after lunch may relate to last night’s dinner, repeated exposure across several days, or a mixed meal with multiple ingredients. A rough food diary helps, but memory, portion size, cooking method, and overlapping foods all limit how much confidence you can place in self-observation alone.
Patterns I often see include:
- Digestive symptoms such as bloating, abdominal discomfort, altered bowel habits, or a feeling of heaviness after meals
- Systemic symptoms such as headaches, fatigue, reduced concentration, or joint discomfort
- Skin symptoms that flare and settle without an obvious immediate trigger
Testing is useful here because it can turn a vague suspicion into a more structured investigation. It does not replace history-taking, symptom review, or a supervised elimination plan. It helps narrow the list of foods that deserve closer attention.
That point matters because method matters. If IgG testing is being used to guide dietary changes, the quality of the sample directly affects how much confidence you can place in the result. Clinical-grade venous blood collection through a pathology setting gives controlled handling, appropriate processing, and better sample integrity than many home collection kits. For patients trying to make meaningful decisions about what to remove and what to keep eating, that difference is practical, not technical.
If you want a clear explanation of the distinction between these reactions, this guide to allergy and intolerance testing is a useful starting point.
A 2022 study summarised by ImuPro Australia reported symptom improvement in participants who followed an elimination approach guided by IgG findings. That does not mean every positive result is clinically relevant, and it does not mean a lab report should dictate your diet on its own. It does support a careful process: use a high-quality sample, interpret the findings in context, then confirm relevance through a structured elimination and reintroduction phase.
The goal is accuracy. A broad list of suspect foods from an unreliable sample can create unnecessary restriction. A well-collected serum sample, interpreted properly, gives a more useful starting point for identifying whether a food is genuinely contributing to ongoing symptoms.
Exploring Clinically Recognised Testing Methods
A patient may react to yoghurt with bloating, wine with flushing, and a mixed meal with symptoms that do not appear until the next day. Those patterns should not be investigated with the same test. The useful question is not "which test is available?" but "which mechanism are we trying to confirm?"
IgG blood serum testing
For delayed reactions, clinical-grade IgG testing uses a venous blood draw and analyses blood serum in a laboratory. That collection method matters. IgG results are only as useful as the sample that reaches the lab.
In practice, venous collection through a pathology setting gives better control over the steps that affect accuracy: correct tube use, proper clotting and centrifugation, temperature handling, transport timing, and traceable processing. Home kits are convenient, but convenience introduces more variables. Capillary collection can be harder to perform correctly, sample volume may be limited, and delays in transit can affect sample quality before analysis even begins.
That trade-off is often underappreciated. If a result is going to shape an elimination plan for several weeks, I want the sample collected under conditions that reduce avoidable error.
IgG testing commonly uses ELISA methodology to assess reactivity across a broad range of foods. It is one tool, not a diagnosis on its own. Used properly, it helps prioritise which foods deserve structured elimination and later reintroduction. For a broader explanation of how these methods differ, this guide to allergy and intolerance testing is a useful reference.
One option in this category is ImuPro Australia, which uses blood serum analysis with pathology collection and laboratory ELISA processing for delayed food reactivity assessment.
If test results will influence what you eat every day, sample integrity should be treated as part of the test, not an afterthought.
Breath testing for lactose and fructose issues
Hydrogen breath testing is better suited to suspected lactose intolerance or fructose malabsorption. It measures a different process entirely. The question here is whether specific carbohydrates are being poorly absorbed and then fermented in the gut.
That distinction matters clinically. If symptoms are predictable, fairly quick, and closely tied to dairy or high-fructose foods, breath testing may give a clearer answer than a broad antibody panel. It is narrower, but sometimes narrower is better.
DAO testing for histamine-related patterns
DAO enzyme testing can add context when symptoms suggest histamine intolerance. The pattern often includes headaches, flushing, skin symptoms, palpitations, nasal congestion, digestive upset, or fatigue after histamine-rich foods.
DAO results need careful interpretation because histamine issues are rarely explained by one marker alone. Still, in the right patient, this testing can help explain why a standard elimination approach has only partly worked.
A simple comparison
| Method | Best suited to | What it helps clarify |
|---|---|---|
| Serum IgG testing | Delayed, broad, hard-to-track symptoms | Foods worth prioritising in an elimination plan |
| Hydrogen breath testing | Suspected lactose or fructose malabsorption | Whether specific sugars are being poorly absorbed |
| DAO enzyme testing | Suspected histamine-related symptoms | Whether histamine handling may need closer review |
How to Prepare for Your Food Intolerance Test
You book a test because symptoms have dragged on for months, then try to be proactive by cutting out the foods you suspect. A week later, your blood is drawn, and the report comes back with less clarity than expected. I see this mistake often. Good preparation improves the odds that the result reflects real exposure rather than an incomplete picture.

The rule patients most often get wrong
Before an IgG antibody test, keep eating a normal, varied diet for 2 to 4 weeks unless a practitioner has given different instructions for a separate medical reason. If you remove foods too early, antibody activity may fall enough to make the report less useful.
Practical rule: Do not start a restrictive diet before an IgG test unless there is another clear medical reason to do so.
This can feel frustrating, especially if one or two foods already seem suspicious. The trade-off is simple. Short-term symptom avoidance can reduce the quality of the information you are paying to collect. For delayed food reactions, recent and regular exposure helps the laboratory measure what your immune system is responding to.
What the collection process should look like
Clinical-grade testing starts with collection quality, not just the lab report at the end. For IgG testing, I advise patients to choose a provider that uses venous blood draw and pathology collection rather than a finger-prick home kit.
The usual process is straightforward:
- Book through a provider using a pathology network so the sample is collected by trained staff.
- Attend the venous blood draw after maintaining your usual diet in the lead-up period.
- Have the sample processed as serum under controlled laboratory conditions with correct labelling, handling, and transport.
If you want more detail on how serum-based analysis is performed, ImuPro’s test method for venous blood serum processing outlines the laboratory pathway.
Why sample integrity matters
IgG results are only as reliable as the sample that reaches the laboratory. That is one reason pathology collection matters so much. Venous blood draw provides a larger, cleaner sample for serum analysis, and the chain of handling is clearer from collection to processing.
Home kits are convenient, but convenience and sample quality are not the same thing. A poorly collected, delayed, or temperature-affected specimen can become the weakest part of the method. In practice, clinical collection reduces avoidable problems with volume, labelling, transport, and specimen stability.
No test becomes accurate just because it is done in a clinic. But if the goal is to make careful decisions from IgG findings, starting with a properly collected venous sample puts the method on much firmer ground.
Interpreting Your Test Results Effectively
You get your report back, scan the coloured results, and want one clear answer: what do I stop eating? In clinic, that reaction is common. It is also where people make their biggest mistakes.
What elevated IgG results actually tell you
An IgG report ranks foods by antibody reactivity. That helps set priorities for investigation, but it does not prove that every flagged food is driving symptoms each time you eat it.
Context matters. A food that appears on a report may be a meaningful trigger, a marker of regular exposure, or a finding with little day-to-day relevance. The job is to sort those possibilities carefully rather than treat the whole report as a ban list.
This is one reason I prefer clinically collected venous serum testing over home kits. If a result is going to influence a restrictive diet, the sample behind it should be as reliable as possible. Poor sample quality creates interpretation problems before the clinical work even starts.
Elevated IgG findings work best as a shortlist for structured testing, not as a permanent list of forbidden foods.
Clinical correlation matters more than colour coding
The report has to fit the patient in front of you. A high reaction to a food you rarely eat is usually less persuasive than a moderate reaction to something you eat daily before symptoms flare. Symptom pattern, exposure frequency, digestive history, skin changes, headaches, fatigue, and bowel habit all matter.
That is why laboratory testing is only one part of the method. The stronger process combines a careful history, a technically sound blood sample, and a structured dietary trial. If you want a plain-language overview of how reports are read, this guide to understanding IgG food sensitivity test results is a useful reference.
A practical review usually asks:
- Timing: Do symptoms appear after the flagged food often enough to suggest a pattern?
- Exposure: Is the food eaten regularly enough to be a plausible contributor?
- Clinical fit: Does the result match the broader picture, or does it look incidental?
- Dietary importance: Will removing it create nutritional or social problems that need planning?
Why self-interpretation often goes wrong
People often focus on the highest numbers and ignore everything else. Clinically, that is too simplistic. Interpretation should weigh reactivity against symptom burden, nutritional value, habitual intake, and the likelihood of getting a clear answer from an elimination trial.
There is also a trade-off. Removing too many foods can reduce symptom noise, but it can also make the diet unworkable and increase the risk of unnecessary restriction. Removing too few may leave the main trigger in place and produce an inconclusive trial. Good interpretation aims for enough precision to test causation without creating avoidable dietary chaos.
Common mistakes after getting results
| Mistake | Why it causes problems | Better approach |
|---|---|---|
| Removing every reactive food immediately | It creates an unnecessarily restrictive diet and makes long-term adherence harder | Prioritise the foods with the strongest clinical relevance |
| Treating the report as a diagnosis | It skips the history, symptom pattern, and real-world response | Use the report to guide a structured elimination and reintroduction process |
| Ignoring how the sample was collected | Lower-quality collection can weaken confidence in borderline findings | Give more weight to results from properly handled venous serum samples |
| Skipping follow-up monitoring | You cannot tell whether symptoms improved because of a specific change | Track symptoms, food intake, and reintroductions in an organised way |
Creating Your Personalised Elimination and Rotation Plan
A good plan is structured, but it shouldn’t be rigid for the sake of it. The purpose is to reduce symptom load, test causation, and then rebuild dietary variety. That usually works best in three phases.
Elimination phase
Begin by removing the foods that are most relevant based on your symptoms, history, and test findings. Keep the diet broad enough to remain nutritionally balanced and realistic.
During this phase, many people make one of two mistakes. They either remove too little and never create a clear therapeutic trial, or they remove so much that the plan becomes unsustainable. The middle ground is where good practice sits.
Key principles include:
- Be selective and prioritise foods that are both reactive and clinically plausible
- Keep records of digestion, energy, skin, sleep, headaches, and bowel changes
- Protect variety by rotating tolerated foods rather than relying on the same few meals
Provocation phase
Once symptoms have settled, foods are reintroduced one at a time. This step matters because it distinguishes laboratory reactivity from real-life symptom provocation.
Reintroduction should be orderly. Change one variable at a time. If several foods come back together, the signal gets muddy and you’re back to guessing.
Reintroduction is where you confirm whether a food is a meaningful trigger, a minor issue, or simply a laboratory finding without strong day-to-day impact.
Stabilisation phase
Long-term eating shouldn’t feel like a punishment. After the most relevant triggers have been identified, the aim is to build a sustainable rotation pattern that supports symptom control while keeping the diet varied.
That often means:
- returning tolerated foods confidently
- limiting only those that consistently provoke symptoms
- spacing out repeatedly problematic foods rather than eating them daily
- reviewing whether extra layers, such as histamine management or gut-focused support, are needed
The best plans are personalised. A person with bloating after dairy and fruit won’t need the same strategy as someone with headaches, sinus symptoms, and reactions to fermented foods.
When to Consult a Healthcare Practitioner
Self-directed testing has limits. If symptoms are severe, persistent, or unclear, professional input matters. A practitioner can help rule out conditions that shouldn’t be missed, including non-food causes of gut symptoms, and can keep any elimination plan nutritionally sound.
That becomes even more important when symptoms are mixed or the first round of dietary changes hasn’t worked. For complex cases, such as suspected histamine intolerance, emerging tools like DAO enzyme testing can provide additional objective data. A qualified practitioner can help integrate these results with IgG findings to create a more nuanced and effective dietary plan, as described on ImuPro Australia’s histamine intolerance test page.
If your symptoms involve significant digestive distress, ongoing fatigue, skin flares, headaches, or multiple suspected triggers, don’t rely on a report alone. Use testing as part of a supervised clinical process.
If you want a pathology-collected, clinical-grade approach to delayed food reactivity assessment, ImuPro Australia provides blood serum IgG testing and complementary diagnostics that can be integrated into a structured elimination and rotation plan with practitioner oversight.